A child who worries before a test, feels shy at a party or wants extra reassurance at bedtime is not automatically experiencing an anxiety disorder. Fear is part of normal development. Concern becomes more important when worry is unusually intense, persists beyond the situation, leads to repeated avoidance or interferes with sleep, learning, friendships or family routines.
Why this pattern happens
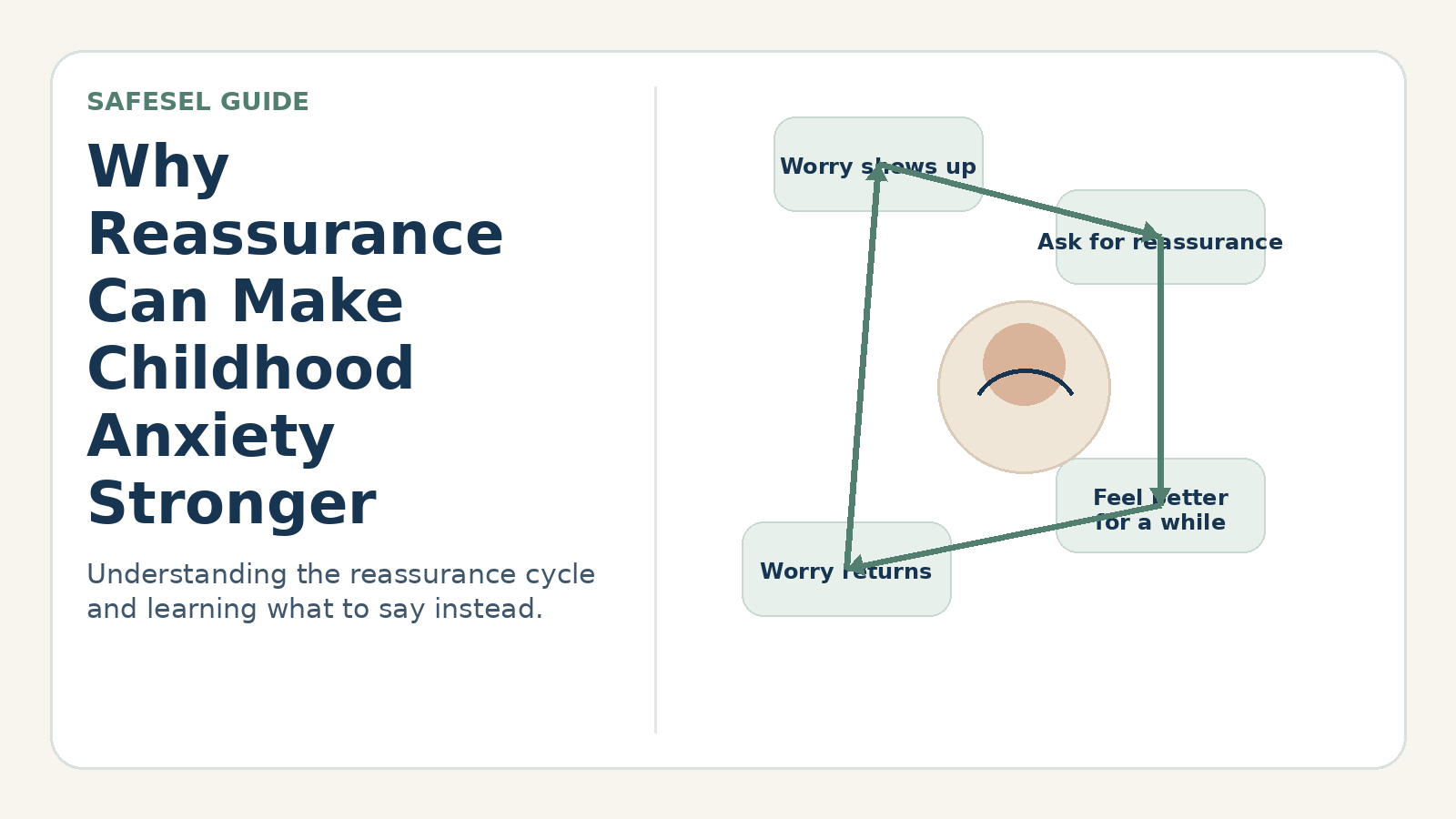
Normal worries usually rise around a real challenge and settle when the challenge passes. Anxiety may continue after reassurance, spread to new situations or make ordinary tasks feel dangerous.
No single checklist can diagnose a child. Temperament, age, culture, neurodevelopment, recent stress and physical health all affect how anxiety appears. The useful goal is not to label quickly, but to notice whether fear is narrowing the child’s life.
Signs and patterns to notice
Patterns matter more than occasional difficult days. Notice what happens across several weeks and in more than one setting.
- Frequent stomachaches, headaches, nausea, dizziness or urgent bathroom visits around stressful events.
- Repeated reassurance questions that return even after a clear answer.
- Avoiding school, activities, sleepovers, speaking, mistakes or separation from a caregiver.
- Difficulty falling asleep because of “what if” thoughts or repeated checking.
- Irritability, tearfulness, freezing or angry outbursts when a feared task approaches.
- Family routines increasingly organized around preventing the child from feeling anxious.
A practical step-by-step response
Track the pattern for two weeks
Write down the trigger, the child’s prediction, body sensations, what the child avoided or completed, and how long recovery took. A brief record is more useful than relying on memory after a stressful day.
Ask about the feared outcome
Instead of only asking “Why are you anxious?”, try “What does your brain think might happen?” The answer often reveals a specific fear such as embarrassment, separation, vomiting, failure or being unable to escape.
Validate without confirming danger
Acknowledge that the feeling is real while keeping the message grounded: “Your body is sending a strong alarm. Let’s check whether this is a danger problem or a worry problem.”
Protect routines where possible
Continue ordinary sleep, school and activity routines with reasonable support. Removing every demand can bring short-term relief while teaching the brain that avoidance was necessary.
Choose one manageable brave step
Break the avoided task into a step the child can repeat. Success means approaching while using support, not feeling perfectly calm.
Helpful words adults can use
- “I believe that the worry feels real, and I also believe you can take one small step.”
- “What is the worry predicting? What facts do we have?”
- “You do not have to get rid of the feeling before you begin.”
- “Let’s notice what helped you cope, not whether you felt zero anxiety.”
Common responses that can make the problem harder
- Calling every worry anxiety or diagnosing from a social-media checklist.
- Giving longer and longer reassurance each time the same question returns.
- Forcing the child into the hardest version of the fear without preparation.
- Allowing anxiety to decide all family routines for an extended period.
How to adapt the approach
Younger children may communicate anxiety through play, body complaints or behavior rather than words. Use simple choices and drawings. Older children can help track predictions, avoidance and outcomes. For neurodivergent children, first check whether sensory overload, unclear expectations or communication demands are contributing to distress.
When to seek additional support
Contact a pediatrician, primary care professional or qualified mental health clinician when fear persists for weeks, causes significant avoidance, disrupts sleep or school, produces frequent physical distress, or affects family functioning. Seek urgent help if the child talks about self-harm, cannot stay safe or has severe sudden symptoms that may require medical assessment.