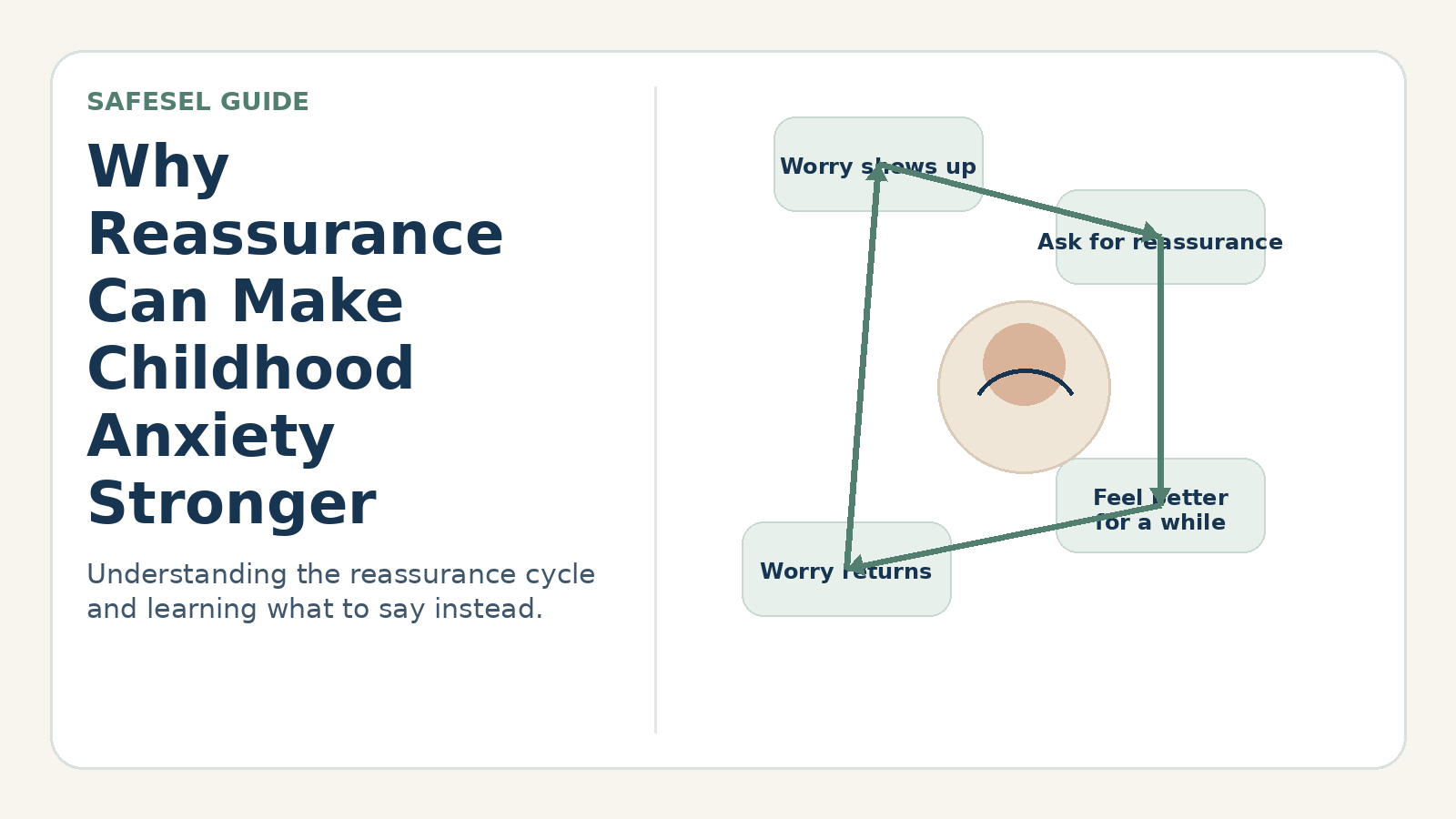
Avoidance makes sense when the brain predicts danger, but repeated escape prevents the child from discovering what they can handle. A fear ladder—sometimes called a brave ladder—turns one overwhelming goal into a sequence of specific, repeatable approach steps.
Why this pattern happens
Gradual exposure is a core element of effective cognitive-behavioral treatment for many anxiety problems. The child approaches a safe feared situation in a planned way and learns that anxiety changes, coping is possible, or the predicted outcome is less likely or less catastrophic than expected.
A worksheet is not a substitute for clinical treatment when fear is severe, complex, trauma-related or linked to medical risk. Adults must confirm that the practice is safe and developmentally appropriate.
Signs and patterns to notice
- The child avoids a clear, safe category of situation.
- The feared goal can be divided into observable actions.
- The child can identify a prediction and rate difficulty with support.
- Avoidance has become broader despite reassurance or preparation.
A practical step-by-step response
Define the target behavior
Use an action such as “answer one question in class,” not a feeling such as “stop being shy.”
List many possible steps
Brainstorm from very easy to difficult. For speaking anxiety, steps might include reading aloud alone, recording a voice note, reading to a caregiver, answering a teacher privately and then speaking in a small group.
Rate difficulty
Use a 0–10 scale and begin around 3–5, depending on the child and clinical guidance. If the child repeatedly cannot begin, reduce the step.
Name the prediction
Before practice ask, “What do you think will happen?” Afterward record what occurred and what the child learned.
Repeat before moving up
Practice across days and contexts. Move upward when the child can complete the step with manageable support, not only when anxiety reaches zero.
Helpful words adults can use
- “Brave means doing the planned step while the alarm is present.”
- “What would make this step smaller without turning it into avoidance?”
- “What did the worry predict, and what actually happened?”
- “We repeat to teach the brain, not to prove you can do everything at once.”
Common responses that can make the problem harder
- Starting with the hardest fear to get it over with.
- Using surprise exposure or removing consent from ordinary practice planning.
- Allowing distraction or reassurance rituals to become conditions for every step.
- Treating a temporary rise in anxiety as evidence that practice failed.
How to adapt the approach
Use pictures, stickers or physical ladder cards for younger children. Older children can design experiments and track predictions. For neurodivergent children, separate anxiety-based avoidance from genuine sensory pain, communication barriers or inaccessible environments.
When to seek additional support
Work with a qualified clinician when anxiety is severe, includes panic or compulsions, follows trauma, involves eating or medical fears, or causes major impairment. Never design exposure around genuine danger, abuse, unsafe environments or medical restrictions.