A child in panic may breathe rapidly, shake, feel dizzy, report chest tightness, cry or say they are dying. These symptoms can be terrifying. Because medical problems can resemble panic, adults should not diagnose a first or unusual episode on their own. When a familiar panic plan is appropriate, calm presence and simple guidance are more useful than a stream of explanations.
Why this pattern happens
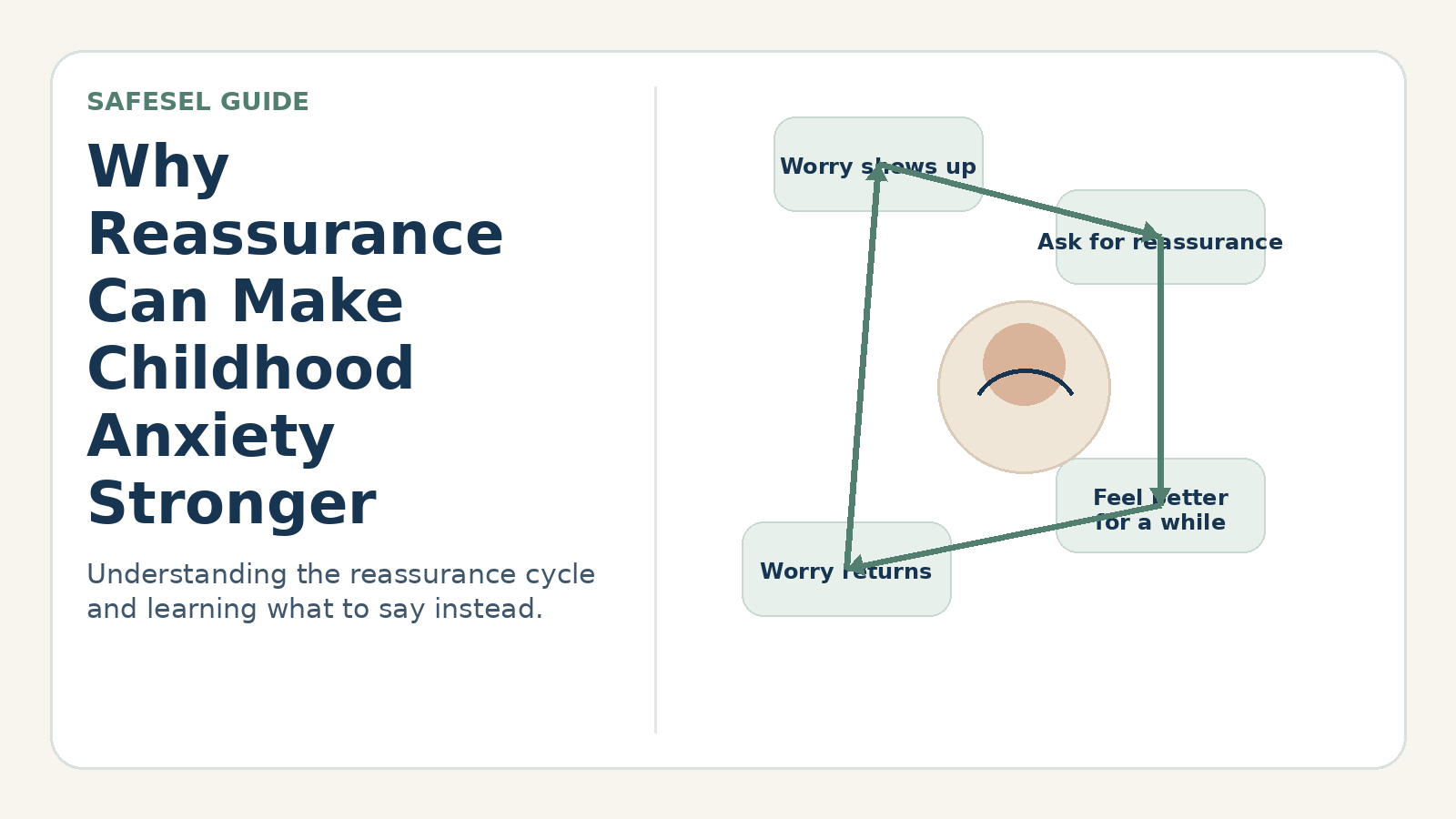
Panic is a rapid surge of intense fear and physical arousal. The child may misinterpret ordinary stress sensations as signs of catastrophe, creating a feedback loop: sensation increases fear, and fear increases sensation.
The immediate goal is safety and orientation. Trying to argue the child out of every fear can overload them. Once the episode passes, a professional can help determine whether it reflects panic, another anxiety problem, a medical condition, substance exposure or something else.
Signs and patterns to notice
- Sudden racing heart, shaking, sweating, dizziness or shortness of breath.
- Chest discomfort, nausea, tingling or feelings of unreality.
- Fear of dying, fainting, losing control or going crazy.
- Strong urge to escape and later avoidance of places where the episode happened.
A practical step-by-step response
Check immediate safety
Follow emergency guidance for severe chest pain, fainting, breathing difficulty, injury, allergic reaction, possible ingestion or symptoms that are new or medically concerning.
Reduce stimulation
Move to a quieter safe space when possible. One calm adult should lead rather than several people asking questions.
Orient to the present
Use concrete observations: feet on the floor, name five visible objects, feel the chair. Avoid making the child breathe into a bag.
Lengthen the exhale gently
Invite a comfortable breath in and a slightly slower breath out, such as cooling soup. Do not insist on very large breaths, which may worsen lightheadedness.
Review after recovery
Record triggers, sensations, thoughts, duration and what helped. Create a written plan with healthcare professionals if episodes recur.
Helpful words adults can use
- “I am here. We will check safety and let the alarm come down.”
- “Feel both feet. Look at the blue chair. Breathe out slowly with me.”
- “You do not have to solve what caused this while your body is at peak alarm.”
- “The sensations were intense. Let’s review them with a professional rather than guessing.”
Common responses that can make the problem harder
- Assuming a first episode is definitely anxiety.
- Crowding the child or asking many rapid questions.
- Promising the sensations can never return.
- Allowing long-term avoidance of every place associated with panic without a treatment plan.
How to adapt the approach
A child with limited speech may use a visual card for pain, breathing and help. Schools should have an individual plan that identifies medical red flags, a calm location and the adult responsible for contacting caregivers or emergency services.
When to seek additional support
Seek urgent medical help for severe or unfamiliar symptoms, loss of consciousness, significant breathing problems, possible poisoning, injury or immediate safety concerns. Recurrent panic-like episodes, anticipatory fear or avoidance should be assessed by a pediatric or mental health professional.