Anxiety is part of normal development. Children may fear separation, unfamiliar people, injury, mistakes, peer judgment or events they cannot control. Concern becomes more significant when fear is intense, persistent or increasingly interferes with sleep, school attendance, learning, friendships, play or family life.
Parents do not need to decide from one behavior whether a child has an anxiety disorder. A more useful first step is to observe the pattern: what triggers the worry, how the child’s body and behavior respond, what the child avoids, how long the difficulty has lasted and whether functioning is changing. Support can then combine accurate information, emotional connection, predictable routines and gradual opportunities to build coping.
In brief: Do not aim to remove every anxious feeling. Help the child understand what is happening, reduce unnecessary uncertainty, and take manageable steps toward safe, age-appropriate activities. Seek qualified assessment when anxiety is persistent, severe or limits daily life.
What Childhood Anxiety Is
Anxiety is an anticipation of threat or difficulty. It may involve thoughts, physical sensations and protective actions. A child might predict that something bad will happen, notice a racing heart or stomachache, and then seek reassurance, escape, freeze or avoid.
This response can be useful. Moderate worry may motivate preparation before a test or caution near danger. The question is not whether the child ever feels anxious. It is whether the response is proportionate to the situation, flexible enough to change and compatible with ordinary development.
Anxiety disorders are clinical conditions that require appropriate evaluation. They are not identified by a printable checklist, a single fear or a parent’s mistake. Physical health, development, learning, environment, family circumstances and other emotional or behavioral concerns may all need consideration.
How Fears May Change Across Ages
Development is variable, so age ranges are guides rather than deadlines.
Ages 4–6
Young children may fear separation, darkness, animals, loud events, imagined creatures or changes in routine. They often communicate through behavior and body complaints rather than detailed explanations. Support is most concrete: visual routines, simple preparation, brief language and repeated practice with a trusted adult.
Ages 7–9
Children become more aware of school performance, rules, injury, peer reactions and real-world dangers. They may ask repeated what-if questions, seek certainty, avoid mistakes or visit the school nurse. They can begin distinguishing a fact from a prediction, but still need adult scaffolding.
Ages 10–12
Concerns about evaluation, belonging, competence, body changes and future outcomes may intensify. Older elementary children may hide anxiety to avoid embarrassment. Perfectionism, procrastination, irritability or refusal can obscure the underlying worry.
The same behavior has different meanings in different contexts. Reluctance at school drop-off during a transition differs from months of school refusal. Consider intensity, duration and interference.
Signs Across Thoughts, Body and Behavior
Thoughts and language
- frequent “what if” predictions;
- expecting the worst outcome;
- fear of mistakes or embarrassment;
- needing repeated guarantees;
- difficulty making ordinary decisions;
- saying a task is impossible before trying.
Physical experiences
- stomachaches or headaches;
- muscle tension or shaking;
- nausea, rapid breathing or racing heart;
- sleep difficulty or nightmares;
- fatigue and trouble concentrating.
Physical symptoms should not automatically be attributed to anxiety. Discuss persistent or concerning symptoms with a healthcare professional.
Behavior
- avoidance of school, peers, sleepovers or new activities;
- repeated checking or reassurance-seeking;
- freezing, crying, irritability or anger near a feared event;
- needing an adult to speak or act for the child;
- perfectionistic overworking;
- escape through nurse visits, bathroom trips or delays.
Quiet, compliant children can also experience substantial anxiety. Absence of disruptive behavior does not mean absence of distress.
Normal Worry or a Pattern That Needs More Attention?
Ask five questions:
- Intensity: Is the reaction much stronger than expected for the situation?
- Duration: Has it persisted rather than easing with adjustment and support?
- Interference: Does it limit sleep, school, play, friendships or family routines?
- Avoidance: Is the child’s world becoming smaller?
- Recovery: Can the child regain functioning, or does each episode shape the rest of the day?
Our focused comparison of normal childhood worry and anxiety that interferes can help parents organize observations, but it cannot provide a diagnosis.
Why Avoidance Can Keep Anxiety Going
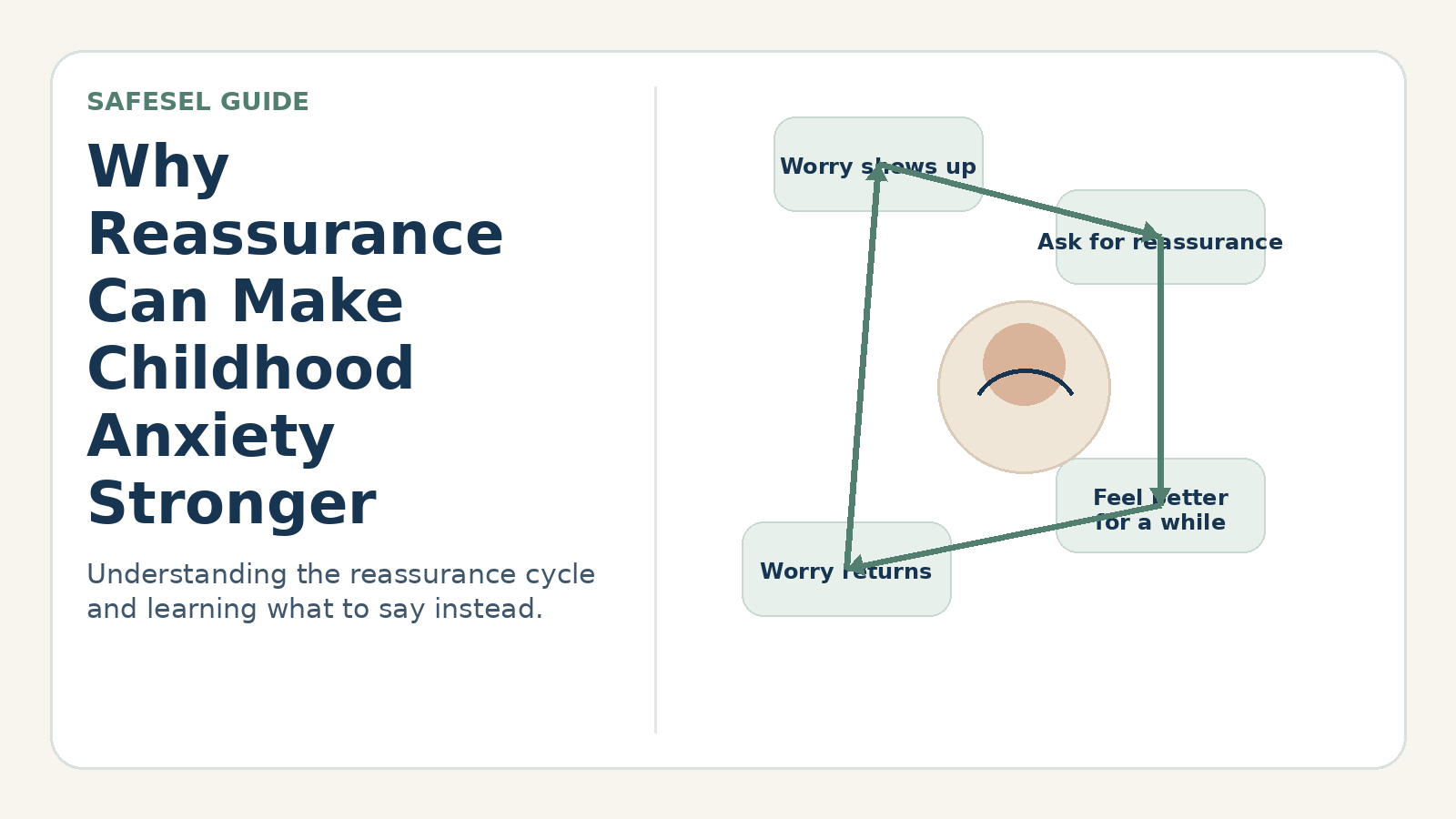
Avoidance often brings immediate relief. A child skips the presentation and the racing heart decreases. A parent answers the worry question again and distress falls. Short-term relief makes the response likely to recur.
Over time, the child receives fewer opportunities to learn that anxiety can rise and fall, that coping is possible or that the predicted outcome may not occur. This is why evidence-informed anxiety treatment often includes gradual engagement with feared but safe situations.
Gradual does not mean forcing. It means matching the step to the child’s capacity, preparing support and repeating manageable practice. Read more about the avoidance and anxiety cycle.
What Parents Can Do
1. Start with accurate information
Clarify what the child genuinely does not know. Describe the school plan, who will help and what happens next. Avoid providing endless guarantees about outcomes nobody can control.
2. Validate the experience without confirming the prediction
Try: “Your body is reacting as if the presentation is dangerous. The feeling is real, and we can make a plan.”
Avoid: “There is nothing to worry about,” or “Yes, everyone may laugh, so you should stay home.”
3. Name the pattern
Help the child connect situation, thought, body response and action. Keep language simple:
“When the teacher announced partners, the worry predicted you would be rejected. Your stomach tightened, and you wanted me to ask for an exemption.”
4. Choose one coping response
Coping may include paced breathing, grounding, a brief coping statement, requesting clarification or using a visual plan. Skills should support engagement, not become rituals the child must perform perfectly before acting.
5. Build a gradual participation ladder
Break a safe goal into steps. For presentation anxiety:
- read the first sentence to a parent;
- practice with the teacher privately;
- present to two peers;
- present one section to a small group;
- attempt the classroom version with a note card.
Steps should be challenging enough to teach something but not so large that practice becomes unmanageable.
6. Reinforce approach and skill use
Notice what the child did:
- “You asked the question yourself even though your voice shook.”
- “You stayed for the first five minutes.”
- “You wanted another guarantee and checked your plan instead.”
Do not require the child to look calm.
Helpful Phrases for Parents
- “You do not have to feel certain before taking one step.”
- “What do we know, what are we guessing, and what can we do?”
- “I can help with the plan; I cannot guarantee every outcome.”
- “The goal is not zero worry. The goal is using support while you participate.”
- “Would you like me beside you or one step away?”
- “What did you learn after trying—not only how anxious did you feel?”
Two Everyday Scenarios
School drop-off
Five-year-old Leo cries at drop-off after a school break. His father begins staying in the hallway until Leo stops crying, which takes longer each day. The family and teacher create a shorter routine: preview the steps at home, one goodbye phrase, a familiar classroom job and a teacher check-in. Leo is allowed to feel upset while practicing separation with consistent support.
For more detail, see separation anxiety at school drop-off.
Homework perfectionism
Eleven-year-old Sam erases every answer and asks whether it is correct. His mother initially checks each line. They switch to one review checklist used once, identify which questions genuinely need clarification and submit the work with some uncertainty. The focus changes from certainty to completing a reasonable process.
Working With School
Share specific observations instead of only saying “My child has anxiety.” Useful information includes triggers, physical complaints, attendance patterns, avoidance, successful supports and changes over time.
Ask what school staff observe across classes and unstructured time. A collaborative plan may include predictable transitions, one identified adult, discreet prompts, gradual participation and a method for reducing support as skills grow.
Accommodations should provide access without automatically removing every challenge. Plans must be individualized and follow school procedures. The AAP emphasizes collaboration among students, families, schools and healthcare professionals when anxiety affects school functioning.
Common Mistakes—Without Blaming Parents
Loving adults understandably try to reduce distress. Patterns that may need adjustment include:
- answering reassurance questions until the child feels certain;
- speaking for the child in every social interaction;
- removing all feared but safe situations;
- surprising the child in an effort to prevent anticipatory worry;
- introducing many coping tools at once;
- debating whether the child “should” feel afraid;
- using worksheets during peak distress;
- treating anxiety as disobedience.
Parents also need support. Consistency is difficult when mornings are rushed or the child is suffering.
Building a Home Plan That Can Be Repeated
A useful home plan is short enough to use on a difficult day. Write down one recurring situation, the child’s first signal, the adult’s response, the child’s coping action and the participation step. For example:
- Situation: Sunday-night worry about school.
- First signal: repeated questions about stomach pain and Monday’s schedule.
- Adult response: answer new information once, validate the discomfort and point to the written morning plan.
- Child action: pack the bag, choose one coping card and complete the usual bedtime routine.
- Participation step: arrive at school and check in with the named adult rather than staying home for familiar anxiety symptoms.
Review the plan weekly, not during every episode. Ask what support helped the child participate and what accidentally prolonged the cycle. Change one element at a time so the family can tell what is useful.
Tracking Progress Without Making Anxiety the Center of Family Life
Parents may track attendance, participation, sleep, reassurance frequency or level of adult support. Choose one or two indicators tied to functioning. Daily symptom interrogation can increase attention to anxiety and make children feel observed.
Progress is rarely linear. A child may complete a presentation and struggle at the next school transition. Look for broader changes: taking steps with less prompting, recovering more quickly, using more flexible language and returning to activities after distress.
Do not interpret a temporary increase in anxiety during gradual practice as automatic failure. At the same time, repeated overwhelming experiences signal that the step, preparation or support needs adjustment.
Questions Parents Can Bring to a Professional
- Which situations show the clearest pattern of interference?
- Are physical symptoms being evaluated appropriately?
- What role should caregivers play in treatment or skills practice?
- Which accommodations provide access, and which may unintentionally maintain avoidance?
- How should home and school respond to reassurance-seeking?
- What changes would indicate improvement or a need to revise the plan?
Bring concrete examples and timelines rather than trying to arrive with a diagnosis. A professional can integrate information from the child, caregivers, school and health history.
When a Strategy May Not Fit
Do not use gradual exposure to make a child tolerate an unsafe situation. Investigate bullying, discrimination, academic mismatch, sensory overload, family stress and physical health concerns. A child with language, learning or neurodevelopmental differences may need adapted communication and environmental support.
Coordinate with the treating clinician if the child already has an individualized anxiety plan. Avoid creating competing reassurance or exposure rules at home.
When to Seek Additional Support
Consult a pediatrician or appropriately qualified mental health professional when anxiety is severe, persistent or worsening; prevents school attendance or ordinary activities; disrupts sleep, eating, friendships or family life; causes frequent physical complaints; or is accompanied by substantial distress. Seek urgent assistance for immediate safety concerns.
Evaluation can distinguish among possible explanations and guide treatment. CDC and AACAP resources note that caregiver involvement is particularly important for younger children, and that effective care should fit the child and family.
Related SafeSEL Resources
- Why reassurance can make anxiety stronger
- Anxiety stomachaches in children
- Social anxiety: helping without speaking for the child
- Bedtime anxiety routine
- Calm Down and Anxiety Unit for Kids
Sources
- American Academy of Child and Adolescent Psychiatry. Anxiety and Children.
- Centers for Disease Control and Prevention. Anxiety and Depression in Children.
- Centers for Disease Control and Prevention. Treating Children’s Mental Health With Therapy.
- American Academy of Pediatrics. Supporting Students With Anxiety in School.
- American Academy of Pediatrics. Anxiety: Pediatric Mental Health Minute.
- National Institute for Health and Care Excellence. Treatment for Children and Young People With Social Anxiety.
- US Preventive Services Task Force. Screening for Anxiety in Children and Adolescents: Recommendation Statement. *JAMA*, 2022.
- Higa-McMillan, C. K. et al. Evidence Base Update: 50 Years of Research on Treatment for Child and Adolescent Anxiety. *Journal of Clinical Child & Adolescent Psychology*, 2016.
SafeSEL resources are educational and are not a substitute for individualized assessment, diagnosis or treatment. If you are concerned about a child’s safety, development or emotional well-being, consult an appropriately qualified professional.